Conditions I treat ..... Limb reconstruction

Limb reconstruction and deformity correction are interchangeable terms often used to describe reconstruction of native limb anatomy without prosthetic replacement. When orthopedic surgeons think of limb reconstruction and deformity correction, the first thing that springs to mind is a cage surrounding a limb (circular fixator). Despite what many orthopaedic surgeons might think, limb reconstruction and deformity correction are more than just applying circular frames...
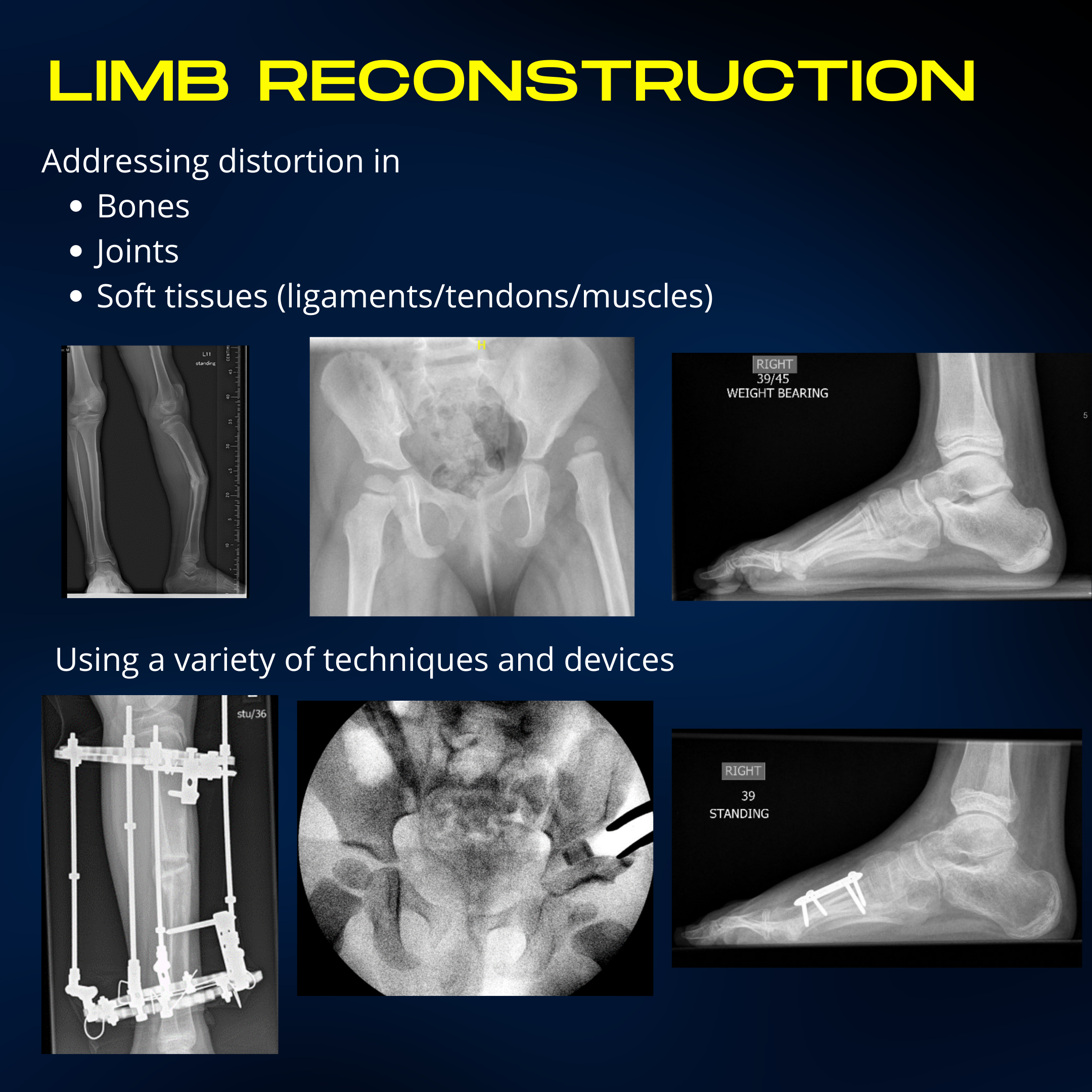
The reality is that all of orthopedics fundamentally relates to deformity correction. The notion that all of orthopaedics can be thought of as deformity correction was first put over to me by one of my trainers. The treatment of every distortion in musculoskeletal anatomy, he argued, could be distilled down to addressing the three main elements - the bones, joints and soft tissues. Deformity correction was thus more than making a bone straight or longer. It encompassed all corrective measures to restore normal bone, joint, muscle, tendon and ligament relationships. Thus, correcting a clubfoot is deformity correction. Addressing a long standing dislocated hip secondary to developmental hip dysplasia is deformity correction. The list goes on......... Ok, I appreciate when doing a hip replacement, cutting out a native hip joint doesn't feel like restoring normal anatomy. However, the principles in terms of correcting vertical and lateral offset, soft tissue balancing and equalisation of leg lengths are core deformity correction principles.
Thinking through pediatric orthopedic conditions using deformity correction principles encourages a holistic approach of how a limb functions. The limb reconstruction/deformity correction surgeon does not consider the lower limb joints in isolation. Correcting any deformity mandates consideration of how the alignment will change upstream as well as downstream. For example, we may lengthen a short femur to equalise leg lengths. However, if we haven't considered that the hip joint above is slightly dysplastic (shallow), then lengthening will likely cause the hip to dislocate as the tension in the surrounding muscles increases. Most surgeons will be aware of at least one patient where this has happened. Similarly we may correct the "bow leg" alignment of a knee but need to be mindful of the effects on ankle alignment. If the ankle alignment is in slight valgus (pointing outwards) then making the "bow leg" straight will likely push the ankle out further making any potential flat foot deformity worse.
The holistic approach of deformity correction extends beyond correcting the bony anatomy alone. If muscle imbalance is a driving force, balance must be restored. If a joint is a distorted by subluxation or abnormally aligned, then we must restore both congruency (appropriate contact between the two surfaces) and stability (i.e. when subjected to normal mechanical forces the joint doesn't dislocate). A good example is hip dislocation in developmental hip dysplasia. An open reduction and capsular reefing may get the hip back in. However, correction of the femoral head coverage with a pelvic osteotomy is what will keep the hip from re-dislocating.
The added challenge in Pediatric Limb Reconstruction is that we are not dealing with a static deformity. In children, the deformity and its response to treatment are continually evolving as the child grows older. Significant deformity, places the limb (like any mechanical system) into a higher state of entropy. The natural laws of the universe dictate that a body in a higher state of entropy inherently moves towards a lower state of entropy unless barriers exist to prevent this (like the Leaning tower of Pisa, each year it shifts a little more). Therefore most, but not all, deformities often increase in magnitude as the child grows older. The situation is made more complex by the fact that the human body, unlike the leaning tower of Pisa, is not inert. Biological systems are adaptive and reactive. In the face of increasing deformity, the body tries to maintain equilibrium by developing compensatory deformities. For example in the high arched foot, the heel compensatorily twists inwards to maintain a stable base of contact. Early on if you correct the arch of the foot, the heel will revert back to it's normal alignment. However, if left untreated the heel stiffens in its altered position. Correcting the foot at a later stage means that once we correct the arch, we unmask the compensatory heel deformity which will also need to be corrected. The best deformity correction surgeons approach deformity like a game of chess - you win by thinking several moves ahead.
Cumulatively putting this complex tapestry together makes one realise that there is very little "fire and forget" or "one off" surgery when it comes to treating complex pediatric deformity. Ultimately, every child with complex lower limb deformity requires a "lifetime treatment plan." The intention is that treatment is planned and staged at appropriate time-points bearing in mind the unique patient circumstances (and often equally unique deformity). The ultimate outcome we are aiming for is equal limb lengths that are well aligned with no joint distortion or muscle imbalance by the time the child transitions into adulthood. This may require several staged surgeries at various time points to achieve this goal and parents need to be counselled well in advance of embarking on this treatment journey.
