Conditions I treat......... Legg-Calve-Perthes Disease

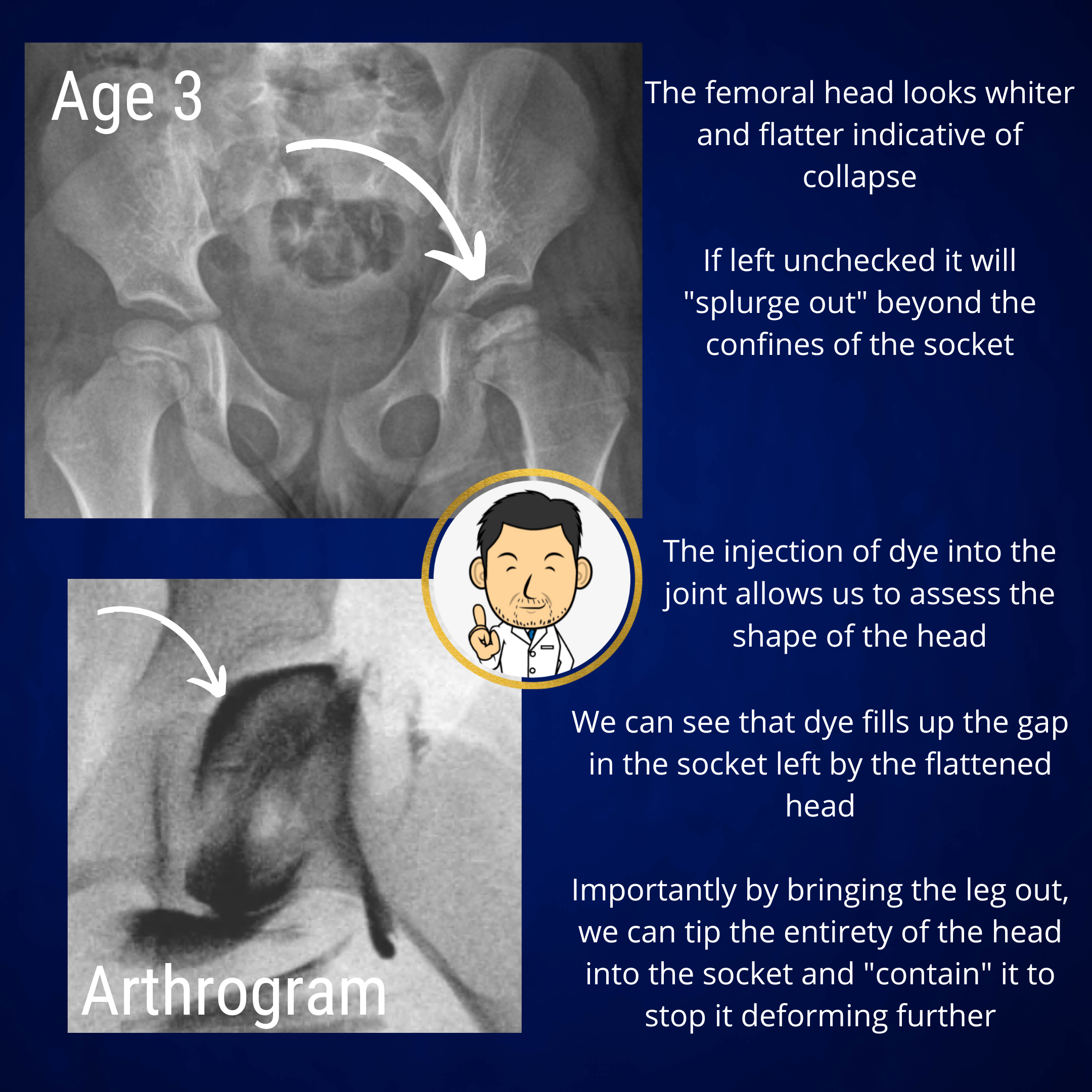
Arthrogram assessment
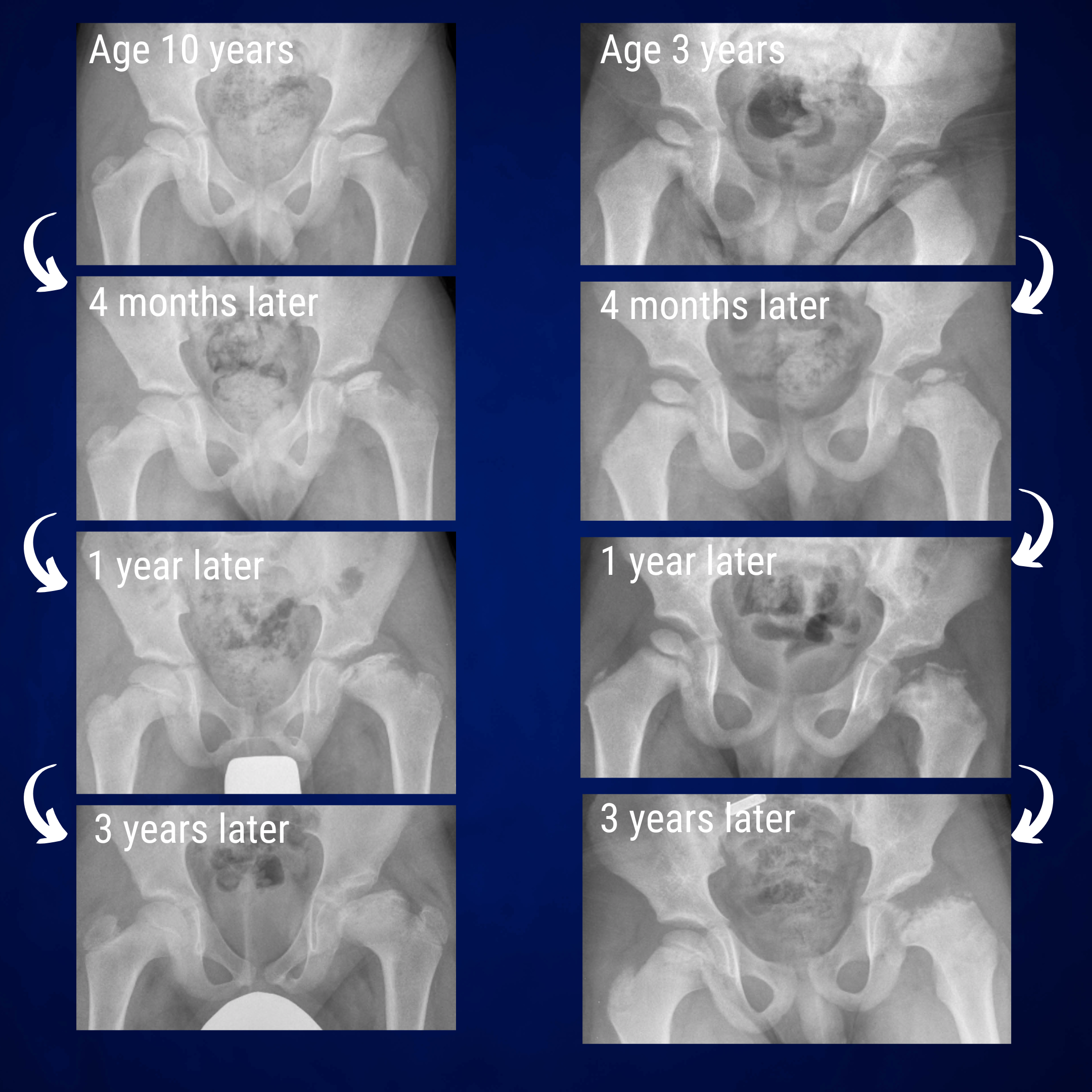
In Perthes disease, the femoral head undergoes progressive structural change ultimately leading to collapse. We don't understand why this happens but likely relates to a disruption in the blood supply to the hip. The pathological process is inexorable and the head undergoes necrosis (bone death), fragmentation, collapse and then regeneration. Fortunately, the femoral head does heal but if the shape is critically deformed as it collapses, the healed femoral head is often oversized and mis-shapen.
The aim of "containment" surgery is to keep the collapsing head completely within the confines of the socket. The ethos is that a "contained" head can not deform into a large mis-shapen head. Surgery to contain the hip is crucially best undertaken before the head shape is critically compromised. If the head has already expanded beyond the confines of the acetabulum, then it can not be contained. Arthrogram assessment is used to delineate the head shape to decide if the head can be "contained" surgically. Usually this is only feasible during the early stages of the disease process so expedient treatment is crucial when considering containment surgery.
Containment surgery
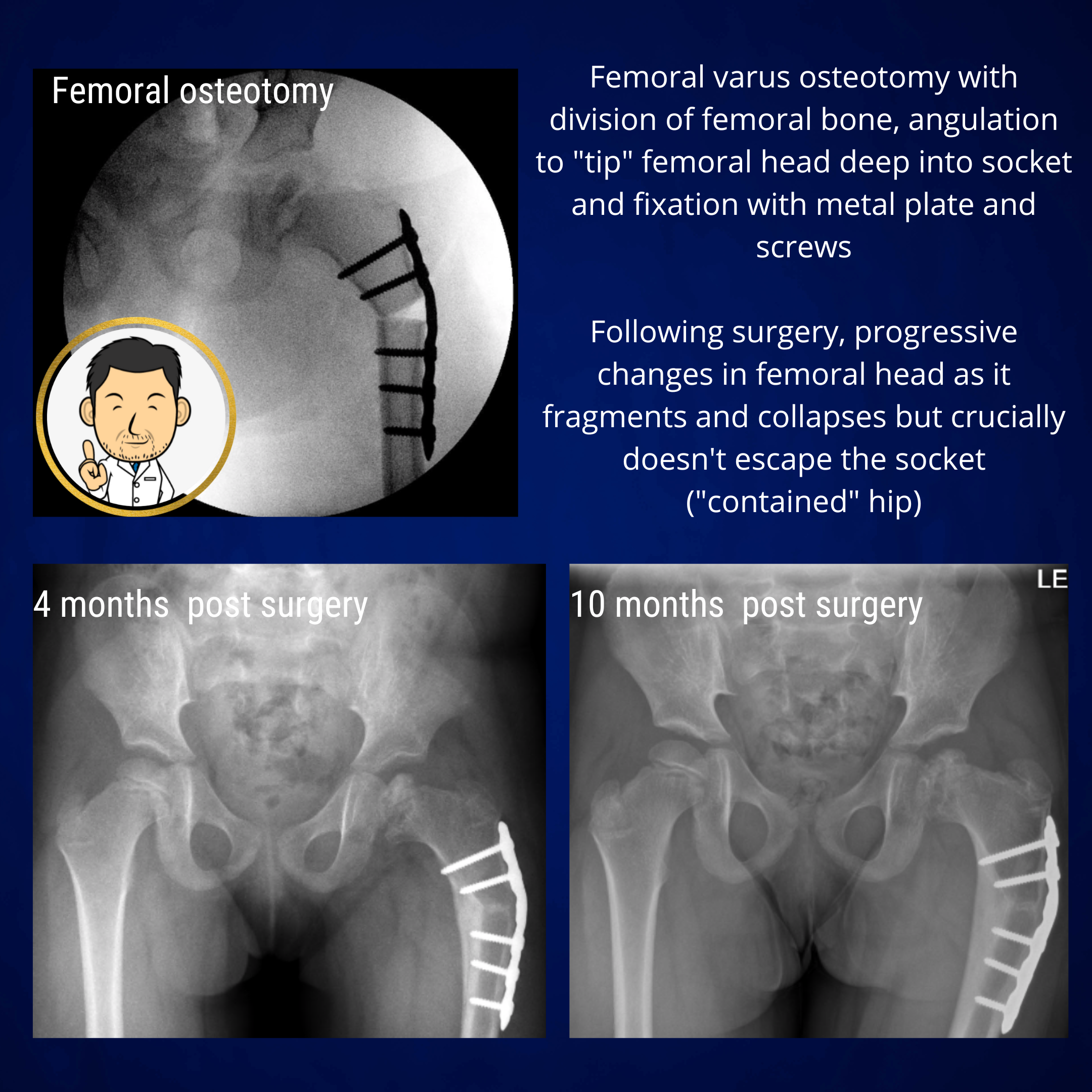
Containment surgery is a good treatment option in the early stages of Perthes disease before significant femoral head deformity has taken place. The aim is to "capture" the head within the socket so that it is confined within the spherical socket and can not deform into a flattened mushroom shape. Containment surgery is usually undertaken with a varus femoral osteotomy (angulation of the top of the thigh bone) to tip the femoral head (ball) deeper into the acetabulum (socket). Hopefully, the contained femoral head will not critically deform as it collapses because it is constrained within the confines of the socket. Therefore as it heals, it can hopefully regain a spherical shape as it should be. Once the head has healed (often several years later) the deformity created by the varus osteotomy can be reversed surgically if required.
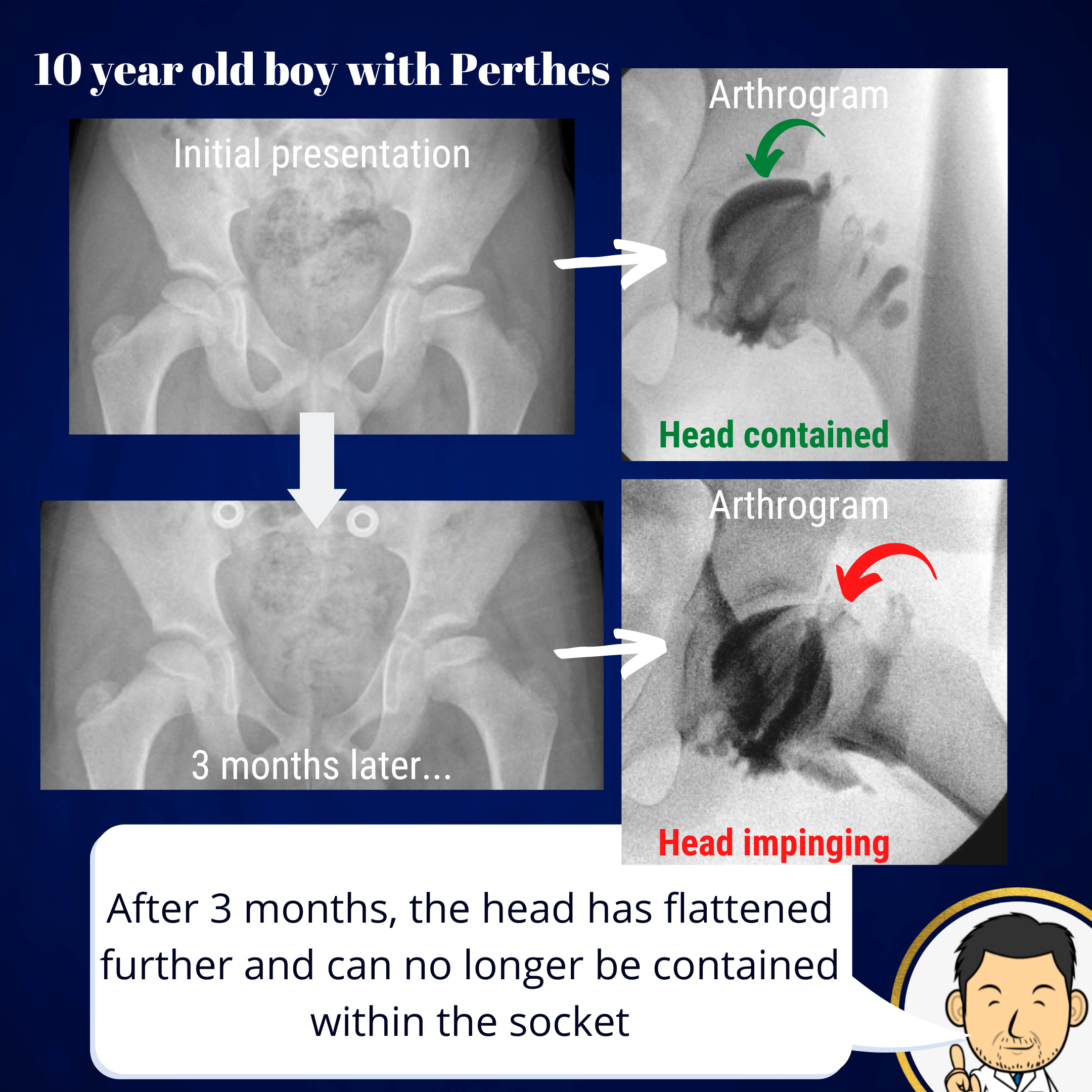
The literature supports timely intervention in Perthes disease. There is a window of opportunity when containment surgery has the greatest chance of success. If left to progress, the femoral head can deform and flatten to a point where it can not fit into the socket to contain it. This is why I advocate early intervention once the diagnosis has been established. Even waiting a few months can change the probability of being able to contain the head.
The scientific literature is undecided on whether surgery will change the outcome in every hip affected by Perthes disease. Proponents of a non-operative approach (mainly physiotherapy and bracing) will highlight cases where the hip underwent progressive collapse and regrowth with a good outcome of a spherical femoral head. Often age is cited as a key consideration in whether to surgically treat. The expectation is that younger patients will have a better outcome given the years of remaining growth that can re-shape the femoral head. However, most pediatric orthopedic surgeons will have encountered cases of young patients with Perthes disease that developed an unfavourable outcome with a flattened femoral head. On this basis, I feel that early surgical intervention to preserve femoral head sphericity is vital to optimise outcomes in patients with Perthes disease. Currently we have no agreed protocol or consensus approach on how to treat the condition. I know colleagues who always undertake containment surgery whilst others prefer to treat with a brace and physiotherapy. All treatment choices should be given to the patient and family for them to decide. My current practice is that containment surgery definitely has a role in influencing the outcome when undertaken early in the disease process.
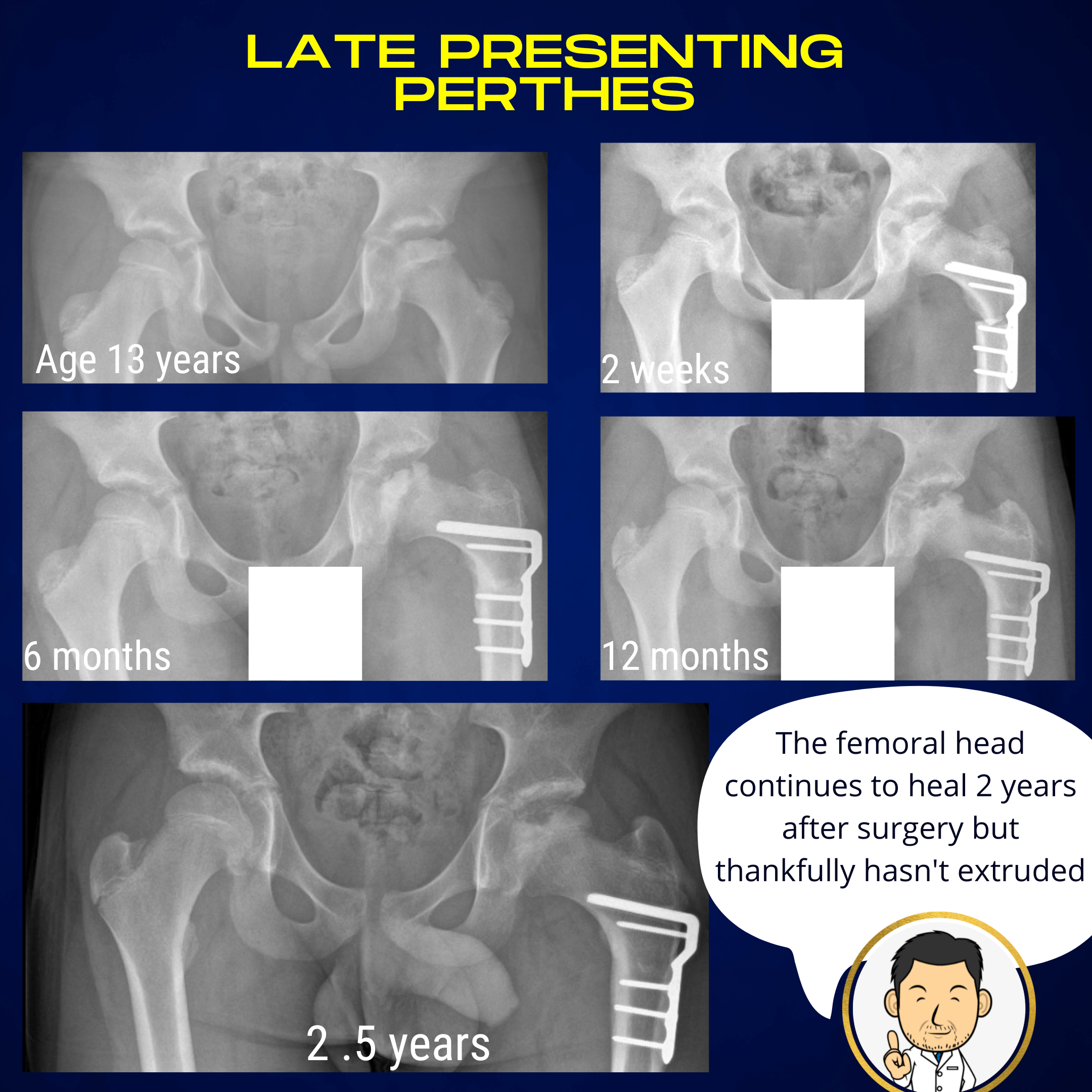
Perthes disease presenting in early teenage years behaves differently to Perthes disease in younger patients. Transition through the distinct stages of collapse and healing may be obscured and it is generally felt that outcomes are less favourable. Early containment may still have a role to prevent the femoral head from flattening and overgrowing the confines of the socket.
Hip distraction
In the later stages of the disease where the head has deformed beyond the confines of the joint, containment surgery may not be feasible or recommended. In such cases there may be a role for a hip distractor. This is an external fixation device which effectively stretches out the hip joint so that the surfaces are not in contact. The ethos is that if you can insulate the weakened femoral head from any compressive forces in the joint, it may limit the extent of further collapse and optimise the chances of sphericity as the head heals.
Deformity correction for healed deformities
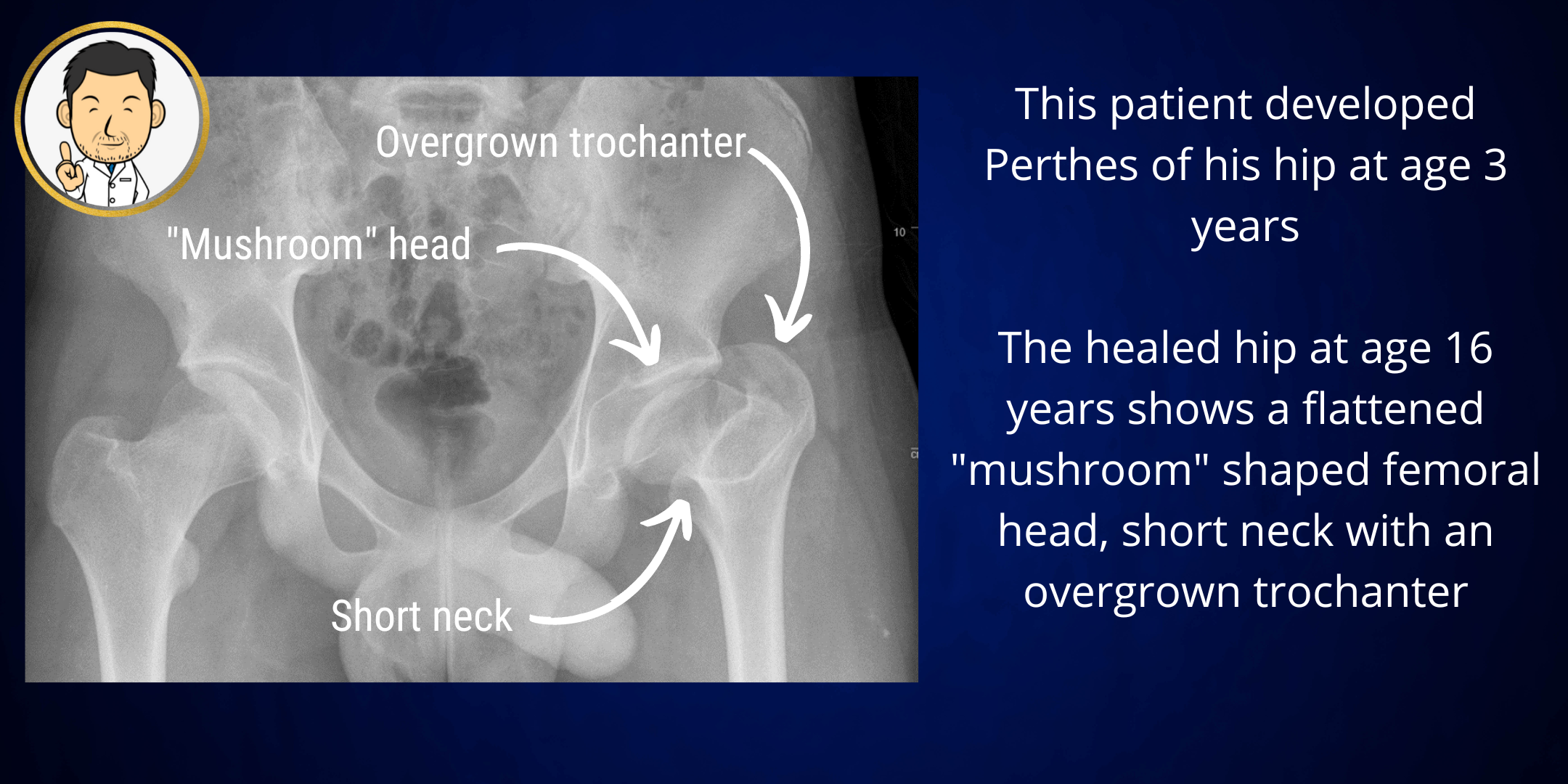
In Perthes disease, the aim of treatment is to optimise the chances of a spherical head at skeletal maturity. In cases where the femoral head is severely involved, the final result after healing may be a flattened head with a short neck and overgrowth of the trochanter (bony prominence where hip muscles attach). In specific patients, there may be a role for a corrective osteotomy to (1) improve the anatomy of the hip and hopefully it's longevity - in effect delay the need for a hip replacement, (2) improve walking ability by restoring the length-tension relationship of the hip muscles and (3) making future hip replacement easier by rendering the anatomy closer to normal. This approach has a role in select cases and is best determined by the treating physician.