Conditions I treat......... Clubfoot

Ponseti Treatment
Ignacio Ponseti, a Spanish Pediatric Orthopedic Surgeon working in Iowa, pioneered a revolutionary technique for treating clubfoot deformity without surgery with superior outcomes back in the 1950s. Unsurprisingly, it took almost 5 decades for his technique to be popularised in the rest of the world (it seems surgeons weren't desperately keen to adopt non-operative treatments). It is very rare in all of Pediatric Orthopedics to have global consensus on the absolute management principles and techniques of a condition. In exacting detail, his treatment protocols for clubfoot are rigorously followed to this day.
I was fortunate to train in Sheffield Children's Hospital where I worked alongside surgeons practicing this technique for the last two decades. To supplement my skillset, I have completed the GCI (Global Clubfoot International) Level 2 Advanced course for clubfoot practitioners. I also presented a scientific paper on my approach to treating clubfoot relapse at the 10th International Clubfoot Congress in Hungary. Suffice to say, it is a condition of great interest to me.
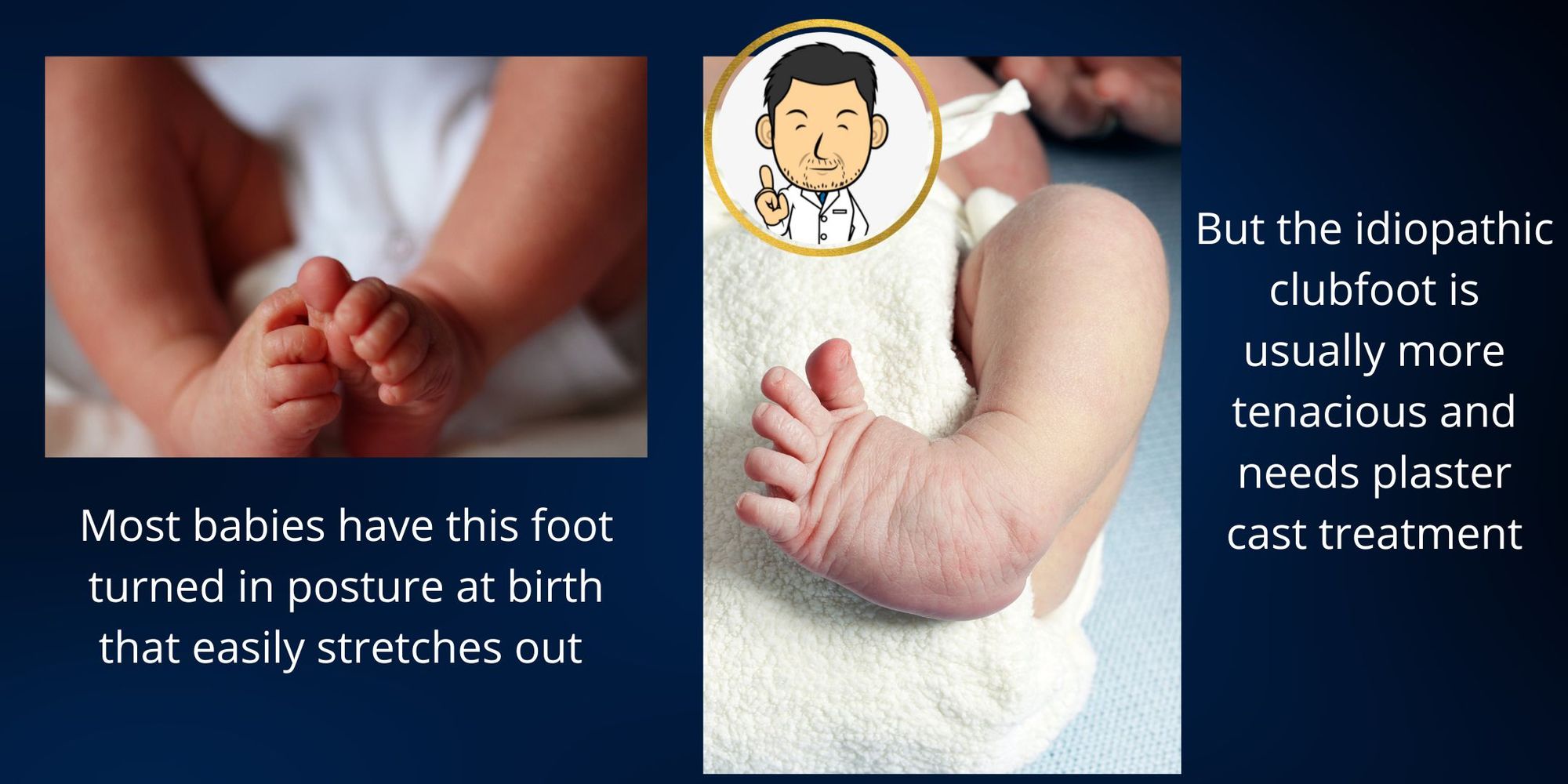
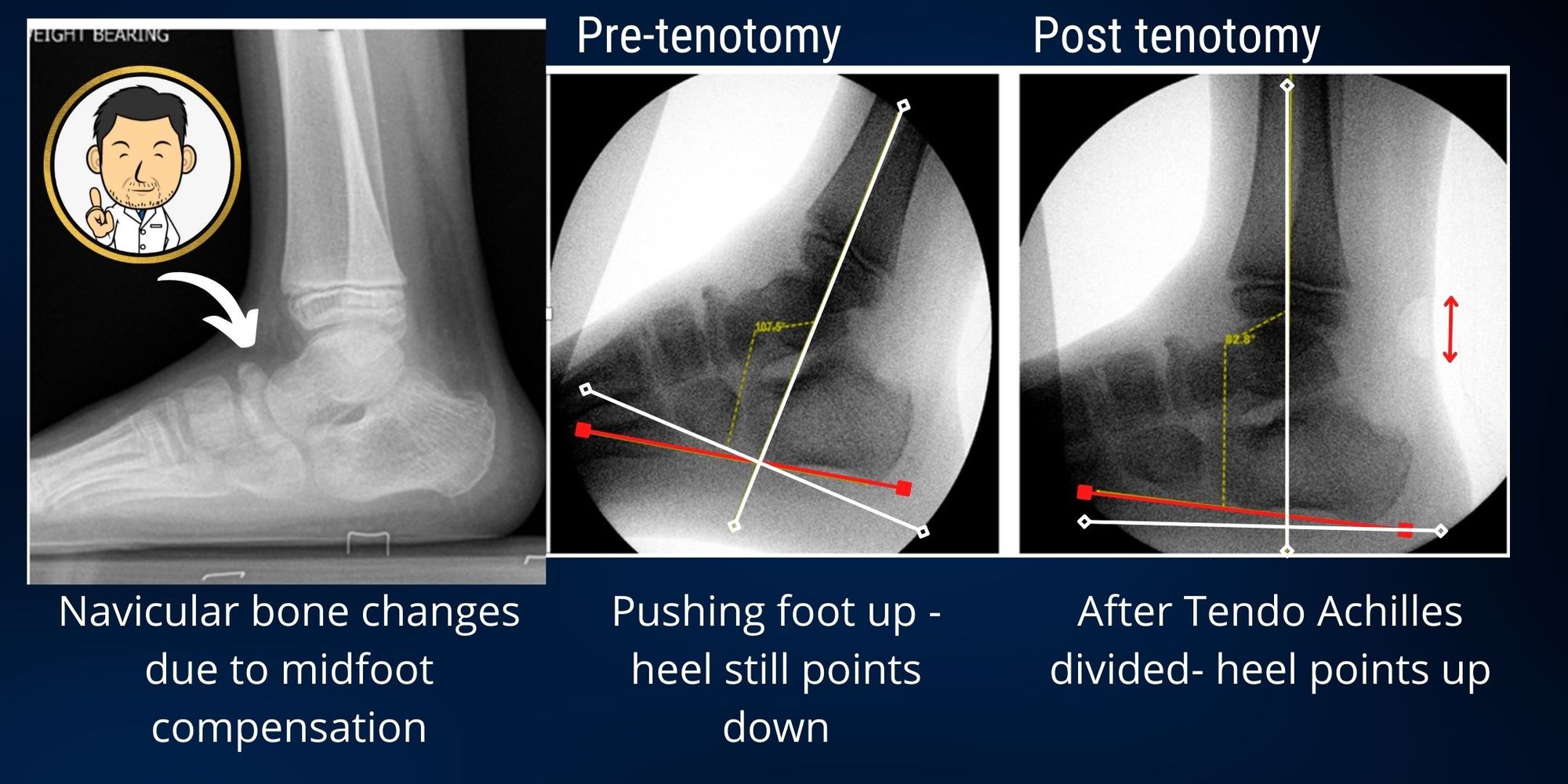
I undertake all the Ponseti manipulations myself on a weekly basis with a trained colleague. The number of casts required can vary depending on the how stiff the deformity is. All patients undergoing treatment for clubfoot are scored using the Pirani Score to assess responsiveness to treatment. Percutaneous Tendo achilles tenotomy is undertaken in clinic before the final cast.
Orthotics
All patients are placed into Boots and Bar following completion of Ponseti serial casting and tendo achilles tenotomy. The boots and bar are fitted by our dedicated Pediatric Orthotist who also renews the boots as the child grows older. I follow up all patients - 3 monthly to the age of 2 years, 6 monthly to the age of 4 years and annually thereafter. I believe it is very important that patients are followed up by a Consultant Pediatric Orthopedic Surgeon who is attuned to looking for predictors for future relapse and also is skilled to detect the earliest signs of relapse which can be quite innocuous to the casual observer.
Treatment for relapse
Relapse (recurrence of clubfoot) deformity can occur in many ways but must be primarly distinguished from insufficient treatment. Often a case will be described as a relapse when in actuality the foot was never completely corrected. This should always raise the question as to whether the clubfoot is atypical (a variant type of clubfoot Ponseti has described requiring a different treatment regimen) or if there is an underlying neuromuscular or syndromic cause.
In all relapses, my over riding principle is not to operate in the first instance (which is strange as it is the antithesis of surgery). My preferred approach is to use serial casting to correct as much of the deformity as possible and then re-assess to detemine the extent of residual deformity and whether surgery is required. Serial casting is both time and labour intensive for a Surgeon but is the safest approach. I also find that doing the serial casting myself each week gives me an instinctive feel for how the foot behaves - which bits are more flexible than others and how willing is the foot to revert back to deformity. Ultimately, serial casting hopes to minimise the extent of surgery required to correct a foot deformity and it is a philosophy I apply liberally when confronted with any clubfoot like deformity. If I can stretch the foot straight then this negates the need for bony corrective surgery to restore alignment. Ongoing growth of the foot as the child grows older can undo the alignment achieved with bony corrcetive surgery or create a new deformity. When it comes to surgery in the growing foot, "less is definitely more".
In most children under the age of 10, where no-one has muddied the waters with surgery, serial casting will correct the alignment of the foot such that only the muscle imbalance driving the deformity needs to be addressed. I usually undertake a tibialis anterior tendon transfer to reduce the pull on the instep and transfer this muscle to bring the foot "up and out" rather than "up and in". I usually perform a tendo achilles tenotomy at the same time to improve the range of ankle movement allowing the transferred muscle to be tensioned to aid the foot "coming up."
Surgical treatment for clubfeet
I do not undertake any open surgery for clubfeet to correct the deformity in the first instance as was done historically before we all learnt from Ponseti that such surgery yielded poor outcomes in the long run. Therefore I do not do any release of the ankle, subtalar or mid-tarsal joints (Cinicinnati approach/Postero-medial release/Postero-medial-lateral release). Every relapse is addressed primarily with repeat serial casting.
Surgery that I do undertake for relapsed clubfeet includes:
- Percutaneous Tendo achilles tenotomy as per Ponseti Technique
- Tibialis anterior tendon transfer as advocated by Ponseti
- Bony correction of any residual deformity after serial casting
Treatment for surgically treated clubfeet
These are very challenging cases and usually require an a la carte approach depending on the type of deformity the foot exhibits. Surgically treated clubfeet may be either under-corrected or over-corrected. The situation is frequently complex as prior surgery induces severe stiffness in many of the mobile joints of the foot which can not be undone by further surgery. Each case must be assessed on an individual basis with treatment aimed at achieving a painfree foot that can achieve flat contact with the ground. It is useful to have all treatment methods at your disposal - serial casting, tendon procedures, bony procedures and circular frame correction. Often waiting until the growth of the foot is complete is best so that we can address a static deformity rather one that may evolve with growth following surgery. However, if the deformity compromises function, then earlier intervention may be required.